Tear Trough Treatment: Why Assessment Matters
Successful tear trough treatment starts with careful assessment. Not every patient with “dark circles” needs tear trough filler, and in fact, treating the wrong patient with filler is one of the easiest ways to create an unnatural or problematic result.
The first question is: is there true hollowing, or is the concern mainly darkness, skin quality, pigmentation, or crepiness?
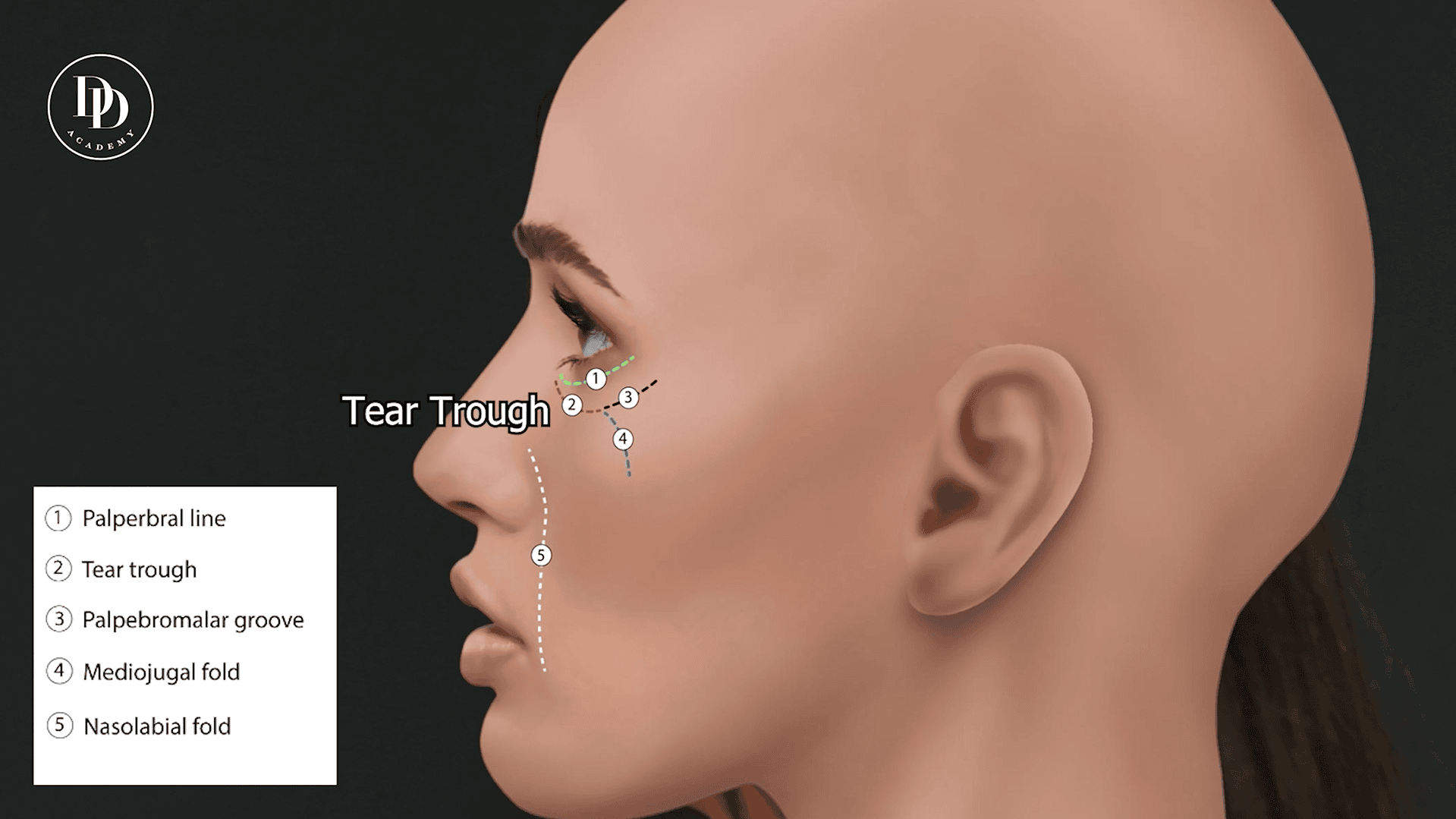
True tear trough hollowing usually occurs when there is volume loss in the sub-orbicularis oculi fat, often referred to as the SOOF. This creates a visible groove or shadow between the lower eyelid and cheek. In these cases, carefully placed tear trough filler can help soften the hollow, support the lid-cheek junction, and reduce the shadowing effect.
However, if the main issue is darkness without hollowing, filler may not be the best option. Darkness can be caused by thin skin, pigmentation, vascular show-through, poor skin quality, or crepiness. In these patients, a regenerative or skin-quality treatment may be more appropriate.
For example, if the under-eye skin is thin, tired-looking, or mildly dark but not hollow, we may use Sunekos, placed superficially in the subdermal plane above the orbicularis oculi muscle, to improve hydration, elasticity, collagen stimulation, and skin brightness.
In older patients with darker, thinner, crepey under-eye skin, polynucleotides may be considered in a similar superficial plane to support tissue repair, improve skin quality, and strengthen the delicate under-eye area over time.
The key point is simple: tear trough filler treats hollowing. It does not treat every type of under-eye darkness.
Choosing the Right Patient for Tear Trough Filler
Tear trough filler can produce beautiful, subtle results when the patient is suitable. However, it is probably one of the easiest filler treatments to get wrong, and the most common reason is poor patient selection.
A good candidate usually has:
- A clear tear trough groove or hollow
- Shadowing caused by volume loss
- Good skin elasticity
- Minimal under-eye puffiness
- No significant malar oedema or festoons
- Realistic expectations
- A desire for subtle improvement rather than complete correction
A less suitable candidate may have:
- Under-eye darkness without true hollowing
- Prominent morning puffiness
- Poor lymphatic drainage
- Malar bags or festoons
- Very thin, loose or crepey skin
- Significant lower eyelid laxity
- Heavy eye bags caused by fat prolapse
- Unrealistic expectations of complete correction
In these cases, filler can sometimes worsen the appearance by adding volume to an area that already holds fluid or has poor drainage.
Why Morning Puffiness Matters
One of the most important questions during assessment is whether the patient wakes up with puffy under-eyes.
If a patient describes regular morning swelling, fluid retention, or puffiness that improves throughout the day, this can suggest poorer lymphatic drainage around the lower eyelid. Tear trough filler, particularly hyaluronic acid filler, can attract and hold water. In patients prone to puffiness, this may increase the risk of prolonged swelling, puffiness, or an overfilled appearance.
This is why we always assess not only the hollow, but also the behaviour of the under-eye area over time.
A patient with a true hollow and no puffiness may be a good filler candidate. A patient with darkness, puffiness, and minimal hollowing may be better suited to skin-quality treatments instead.
The Snap Test: Assessing Lower Eyelid Support
The snap test is a simple clinical assessment used to evaluate lower eyelid tone and skin elasticity.
To perform the test, the lower eyelid is gently pulled downward and then released. In a patient with good eyelid tone, the lid should “snap” back quickly into its normal position. If the eyelid returns slowly, remains distracted, or needs a blink to reposition, this may suggest reduced lower eyelid support or laxity.
This matters because patients with poor eyelid tone, loose skin, or weak support may be more prone to swelling, irregularity, or an unsatisfactory result after tear trough filler.
The snap test is not used in isolation, but it forms part of a broader assessment that includes skin quality, lid-cheek anatomy, hollowing, puffiness, facial structure, and medical history.
When Tear Trough Filler Is Appropriate
Once we have confirmed that the patient has true hollowing and is a suitable candidate, tear trough filler can be used to soften the groove and improve the transition between the lower eyelid and cheek.
At Clinic Dr Dray, the goal is always subtle correction. The under-eye is a delicate area, and overfilling can quickly make the result look puffy, heavy, or unnatural.
For this reason, we usually tell patients to expect a 25–50% improvement, not a complete erasure of the tear trough. The aim is to look fresher and less tired while still looking completely natural.
Our Tear Trough Filler Technique
For true tear trough hollowing, we usually use a cannula technique rather than a needle. A cannula is a blunt-tipped instrument that allows controlled placement of filler through a small entry point, helping the practitioner treat the area carefully and conservatively.
A commonly used approach is a 50 mm, 23G cannula, which allows access to the medial tear trough from a safe and controlled entry point placed within reach of the target area.
The filler we often choose is Teosyal Redensity II, a hyaluronic acid filler specifically designed for the under-eye region. It is soft, smooth, and well suited to delicate tissue, making it a good option for subtle correction in this area. It can also be gently massaged and refined after placement, which is important in such a fine anatomical zone.
The filler is placed deep, beneath the orbicularis oculi muscle, rather than superficially in the skin. This helps support the hollow from underneath and reduces the risk of visible lumps or a bluish Tyndall effect.
Treatment is performed gradually, using very small amounts. Rather than placing large volumes at once, we typically place around 0.1 ml at a time, then withdraw, massage gently, and reassess the improvement.
The maximum amount is usually conservative — often no more than around 0.5 ml per side, depending on anatomy. In many patients, less is needed.
In tear trough treatment, it is always better to undertreat than overtreat. Additional product can be added later if appropriate, but overcorrection can be difficult to manage and may create puffiness or an unnatural appearance.
Why Conservative Treatment Gives Better Results
The tear trough is not an area where more filler means a better result. In fact, the opposite is often true.
Too much filler can create:
- Puffiness
- Visible swelling
- A heavy under-eye appearance
- Irregularity
- A bluish hue under the skin
- An unnatural transition between the eye and cheek
A refined result comes from placing the right product, at the right depth, in the right patient, using the smallest effective amount.
This is why patient selection, anatomy, product choice, and restraint are so important.
Tear Trough Filler vs Sunekos vs Polynucleotides
At Clinic Dr Dray, we do not treat every under-eye concern in the same way.
If the issue is true hollowing, tear trough filler may be the most appropriate option.
If the issue is darkness, thin skin, fine lines, or mild crepiness without hollowing, Sunekos may be more suitable. Sunekos is placed superficially above the orbicularis muscle and works by improving hydration, elasticity, and collagen stimulation rather than adding volume.
If the patient has older, thinner, crepey, or more fragile under-eye skin, polynucleotides may be recommended to support regeneration, tissue repair, and skin quality over time.
In some cases, a combination approach may be best. For example, a patient may need a small amount of deep tear trough filler to improve hollowing, alongside Sunekos or polynucleotides to improve skin quality.
The best results often come from understanding which layer of the under-eye is causing the problem.